Carotid Disease
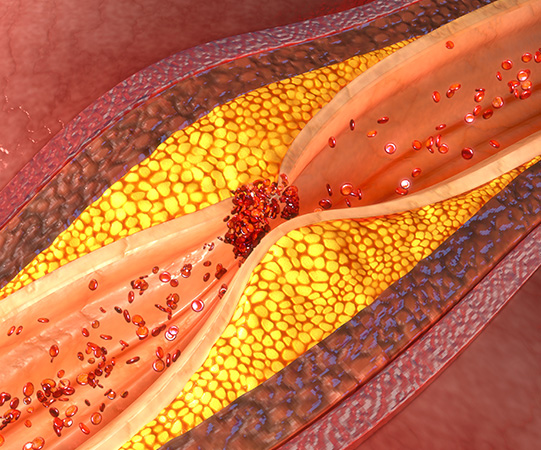
Atherosclerosis, also known as “hardening of the arteries”, a disease in which fat, cholesterol and calcium (plaque) build up inside the vessels that carry blood around the body (arteries). Over time plaque hardens causing narrowing of the vessels and limits the flow of blood. When it effects the carotid arteries in the neck that carry blood to the brain, it can cause stroke. People who suffer a stroke develop weakness down one side, drooping of the face and problems with their speech, vision or thinking. Stroke is a common cause of disability and death.

Carotid disease is associated with increasing age, smoking, high blood pressure, high cholesterol, diabetes and heart disease. Some patients will have a noise in the neck associated with the disturbed blood flow. Before a major stroke some patients have symptoms such as transient loss of vision in one eye from which they recover. Many will however have no symptoms. People who have suffered a stroke should be investigated for the presence of carotid disease.
Ultrasound is the best way to identify patients with atherosclerosis involving the carotid arteries and determine the severity of the narrowing and thereby the risk of stroke. Ultrasound is a non-invasive test that uses high frequency sound waves to obtain images or extent of the disease. It is not painful and does not require any injection or radiation. Ideally it should be performed by an experienced vascular sonographer who understands the assessment of patients with carotid disease. It does however only examine the carotid arteries in the neck, additional studies may be required to examine the arteries in the brain.
All patients should be checked for diabetes and have their blood pressure and cholesterol under control and regularly checked by their GP. Smokers will benefit from quiting. Your GP can discuss with you being on a blood thinner, for example aspirin, to reduce the risk of stroke. Some patients benefit from surgery to clean out the carotid artery (carotid endarterectomy) in order to prevent further damage to the brain after a stroke or to help prevent a stroke in the first place. The decision perform surgery is based on several factors including the degree of narrowing.
Any procedure on the carotid arteries carries with it the risk of causing a stroke. This needs to be balanced against the risk of stroke without surgery which is particularly high in patients who have already suffered damage to the brain. Surgery also carries with it the risk of injury to the nerves that control the tongue, speech and swallowing however these nerves usually recover. There is also the risk of bleeding, especially given that patients need to continue aspirin around the time of surgery. Infection rarely occurs and in some patient’s blood pressure is difficult to control after surgery.
Stenting is a newer procedure that involves placing a scaffold across the narrowing. It is a minimally invasive procedure carried out under local anaesthetic through the groin. In addition to stroke, complications of stenting include damage to the artery in the groin used to place the stent. Not all patients are suitable for stenting. In addition to ultrasound further testing is usually required to determine if stenting is a reasonable alternative. Dr Freeman can discuss the most suitable options for each individual and has extensive experience in treating patients with carotid disease with surgery and stenting.
Aneurysms
Blood vessels, particularly arteries, can develop aneurysms. This involves destruction and weakening of the vessel wall so that it dilates (expands) to become larger than normal. In advanced cases aneurysms can rupture and patients can bleed internally. The vessel most affected is the aorta, the main artery that carries blood from the chest, through the abdomen and down to the legs. A ruptured aortic aneurysm is a life-threatening event that usually has a catastrophic outcome. Aneurysms can also occur in the legs and elsewhere.

Blood vessels, particularly arteries, can develop aneurysms. This involves destruction and weakening of the vessel wall so that it dilates (expands) to become larger than normal. In advanced cases aneurysms can rupture and patients can bleed internally. The vessel most affected is the aorta, the main artery that carries blood from the chest, through the abdomen and down to the legs. A ruptured aortic aneurysm is a life-threatening event that usually has a catastrophic outcome. Aneurysms can also occur in the legs and elsewhere.
Men over 65 years old are most at risk although women and younger people can also develop an aneurysm. People who have relatives with aneurysm, have high blood pressure or cholesterol, and who have smoked are also at increased risk of aneurysm. Aneurysms are four times more common amongst smokers than non-smokers and people with aneurysm who smoke should consider stopping. Once the aortic wall is damaged it will usually continue to increase in size over time.
Most aortic aneurysms cause no symptoms and are discovered incidentally by examination or on X-rays however some people may get pain from their aneurysm. Severe pain and collapse occurs when an aneurysm ruptures. This is an emergency and most people don’t survive. Aneurysms can also develop blood clots which can move to the legs and compromise the circulation. For these reasons when aneurysms are detected consideration needs to be given to repairing them to prevent these problems.
Ultrasound is the best way to detect an aneurysm in order to be able to repair it before it ruptures. Elderly men who have smoked should consider having an ultrasound and anyone with a family history should discuss this option with their GP or Specialist. An ultrasound will provide an accurate assessment of the size of the aneurysm and the risk of rupture. Computed tomography (CT) is the best test to examine an aneurysm before repairing it.
As aneurysms get bigger the risk of rupture increases. When the risk of rupture is greater than the risks associated with repairing an aneurysm then patients should consider having their aneurysm repaired. This typically is the case when the aneurysm is greater than 5 cm in diameter as approximately 10% will rupture each year. It does however also depend on how your health is otherwise, particularly if you also have heart or lung problems. Painful aneurysms should ideally be repaired as they have the greatest risk of rupture.
If you smoke, then you should consider quitting. You should also see your GP to make sure your blood pressure and cholesterol are under control. Unfortunately, there are no drugs that will stop an aneurysm from growing. You should also discuss with relatives whether they need to be checked for an aneurysm particularly if there is a family history. You should have ultrasound surveillance performed by an experienced vascular sonographer to monitor growth, either each year or every six months depending on the size of the aneurysm.
There are two methods to repair an aneurysm to prevent it from rupturing. In the past all aneurysms were repaired by open surgery through a large incision in the abdomen. These days most aneurysms can be repaired using minimally invasive keyhole surgery through the groins. This is called endovascular aneurysm repair (EVAR). Stents are used to reline the aorta and protect the aortic wall from rupturing. Endovascular aneurysm repair is effective and safe in selected patients with fewer risks than open surgery. It is still however a major operation done under general anaesthesia in hospital. Patients need to have their health optimised before proceeding with any aortic procedure.
As with any surgery there comes risks, infection and blood clots can occur. Patients will receive medication to help prevent these complications. Additional stress placed on the heart can trigger a heart attack particularly in patients with existing heart conditions. Damage can also occur to the kidneys, the groin arteries used to access the aneurysm or a leak can develop around the stent used to repair the aneurysm however it is rare that patients do not survive the procedure due to complications.
Patients can expect to spend a few days in hospital following surgery and you will need to have a CT scan to confirm a successful repair. In rare cases, over time the stents can move, or a leak may develop. For this reason, patients should continue to follow up with their surgeon as an ultrasound can usually detect these problems. It is generally accepted that regular surveillance after endovascular aneurysm repair should be lifelong.
Peripheral Artery Disease
Atherosclerosis, also known as “hardening of the arteries”, is a disease in which fat, cholesterol and calcium (plaque) build up inside the vessels that transport blood around the body (arteries). Over time plaque hardens causing narrowing of the vessels and limits the flow of blood. Vessels severely affected can become completely blocked. When it effects the peripheral arteries in the legs it can cause problems walking, pain in the legs and feet, ulcers and in advanced cases gangrene. Patients with peripheral arterial disease are also at risk of heart and carotid disease.
Some things that cannot be changed, such as male gender and advanced age, are associated with peripheral arterial disease. Modifiable risk factors that can be addressed include being overweight, high blood pressure, high cholesterol and high blood sugar in patients with diabetes. Smoking is also a risk factor and patients should carefully consider the benefits of quitting, especially if they require procedures to help restore the blood supply to the legs as these are much less likely to work in active smokers, seek advice from your GP.
Identifying patients with blocked arteries in the legs can be done by measuring the blood pressure at the level of the ankles and comparing it to the blood pressure in the arm (ankle-brachial pressure index). This test has limitations especially in patients with heavily diseased arteries and with diabetes. More detailed information can be obtained with an ultrasound scan. Ultrasound is a non-invasive test that uses high frequency sound waves to obtain images or extent of the disease .It is not painful and does not require any injection or radiation and performed by an experienced vascular sonographer.
Pain in the leg muscles that occurs when walking and is relived with rest (intermittent claudication) is a common problem in patients with peripheral arterial disease. This can be especially problematic when walking uphill and for some patients can significantly limit their mobility. In more advanced cases patients can experience pain when resting and particularly at night, ulcers and gangrene. If not appropriately treated to restore blood flow to the leg, a proportion of patients will go onto require amputation of the leg. Patients with uncontrolled diabetes, those on dialysis and active smokers are at highest risk. Early identification of patients at risk is essential to avoid these devastating complications.
The most important thing is to address the causes of peripheral arterial disease outlined above. Simple measures such as losing weight through diet and exercise are important.
Patients with intermittent claudication should continue to walk regularly and need to understand that although they will still continue to experience pain, damage is not being done to the leg. Patients should also discuss with their GP the potential benefits of being on aspirin to thin the blood and reduce the risk of blood clots. Patients should also consider being investigated for heart and carotid disease as the causes of peripheral arterial disease and heart and carotid disease are the same.
Intervention for peripheral arterial disease has traditionally involved open vascular surgery, such as endarterectomy to clean out the artery directly or bypass to restore flow beyond the blockage. However, more recently the development of minimally invasive keyhole surgery (endovascular surgery) through the groin allows for restoration of flow through angioplasty, where balloons are used to open the arteries, and stenting (inserting a scaffold), where a scaffold is used to hold arteries open. A patients’ suitability for open vascular surgery or endovascular surgery depends on a detailed examination of the arteries using angiography where dye is used to image the arteries.
Open vascular surgical operations are major procedures. Careful consideration needs to be given in relation to the risks versus the benefits. There can be complications such as infection, failed grafts, development of blood clots or heart and lung problems. Complications are more likely to occur ally in patients who continue to smoke.
Minimally invasive endovascular surgery has fewer risks, but complications can occur including damage to the groin arteries accessed during the procedure and kidney damage from the dye used to image the arteries. Dr Freeman has extensive experience in managing patients with peripheral arterial disease and can advise whether you are best treated non-operatively, with surgery or with endovascular treatment.
Mesenteric & Renovascular Disease
The mesenteric arteries supply blood to the bowel in the abdomen and can be affected by several diseases that can compromise blood flow. Complications can arise as a result of blood clots from the heart, especially in patients with abnormal heart rhythms (atrial fibrillation), atherosclerosis or “hardening of the arteries” causing blockage of the arteries, aneurysm where the artery is weak and dilated, or a dissection where there is a tear in the vessel wall that can compromise blood flow.
Sudden blockage of the mesenteric arteries is a medical emergency that requires immediate attention. Patients may experience severe pain, diarrhoea and vomiting. Early recognition is important to avoid gangrene of the bowel requiring major surgery in order to remove the bowel. Patients diagnosed too late are unlikely to survive. Restoring blood flow to the bowel is a priority in these patients. It can be performed using either an open surgery approach or a minimally invasive endovascular procedure through the groin.
More gradual blockage of the artery over a period of months or years can cause pain associated with meals, weight loss and diarrhoea. The typical patient is a female smoker around the age of 60 years old and in contrast to patients with cancer, patients still feel hungry. The reason that the patient doesn’t eat, or eats only very small meals, relates to fear of the pain that comes after the meal. There are several alternative causes for abdominal pain and Dr Freeman can advise if you may benefit from treatment.
Ultrasound can be used to identify patients with blocked mesenteric arteries. Should this be thought to be the cause of a patients’ pain, and no other explanation has been identified despite extensive testing, treatment is aimed at restoring flow to the bowel. This can be achieved with a bypass. However, these days minimally invasive stenting (inserting a scaffold) where a scaffold is inserted to open the artery is preferred in most patients. After stenting patients need to be on aspirin and should quit smoking.
Atherosclerosis or “hardening of the arteries” narrowing the renal vessels that supply blood to the kidneys can cause significant complications including failure of the kidneys to the point that patients require dialysis, and high blood pressure that can be especially difficult to control. Ultrasound scanning can identify renal artery narrowing. Most patients can be managed with medication including aspirin and drugs to reduce cholesterol and blood pressure. Patients who smoke should stop.
A proportion of patients benefit from improving flow to the kidneys by way of a stent (a scaffold) that is delivered through the groin to open the artery. Not all patients are appropriate for stenting and additional tests are usually required to identify which patients will benefit. If a kidney has already completely failed, it will not recover with stenting. Patients have two kidneys, and some require stenting of both renal arteries. Dr Freeman is experienced in treating appropriately selected patients with renal stents.
The renal arteries can also be affected by an aneurysm where the wall is weakened and the artery dilates so that it is larger than normal. Renal artery aneurysms are rare and the risk of rupture is low when they are small. Most patients simply require surveillance with ultrasound. Larger aneurysms may warrant treatment which these days is usually through a minimally invasive endovascular procedure through the groin. Dr Freeman can discuss with you what the options are for treatment.